Primary level management of eye injuries
Related content
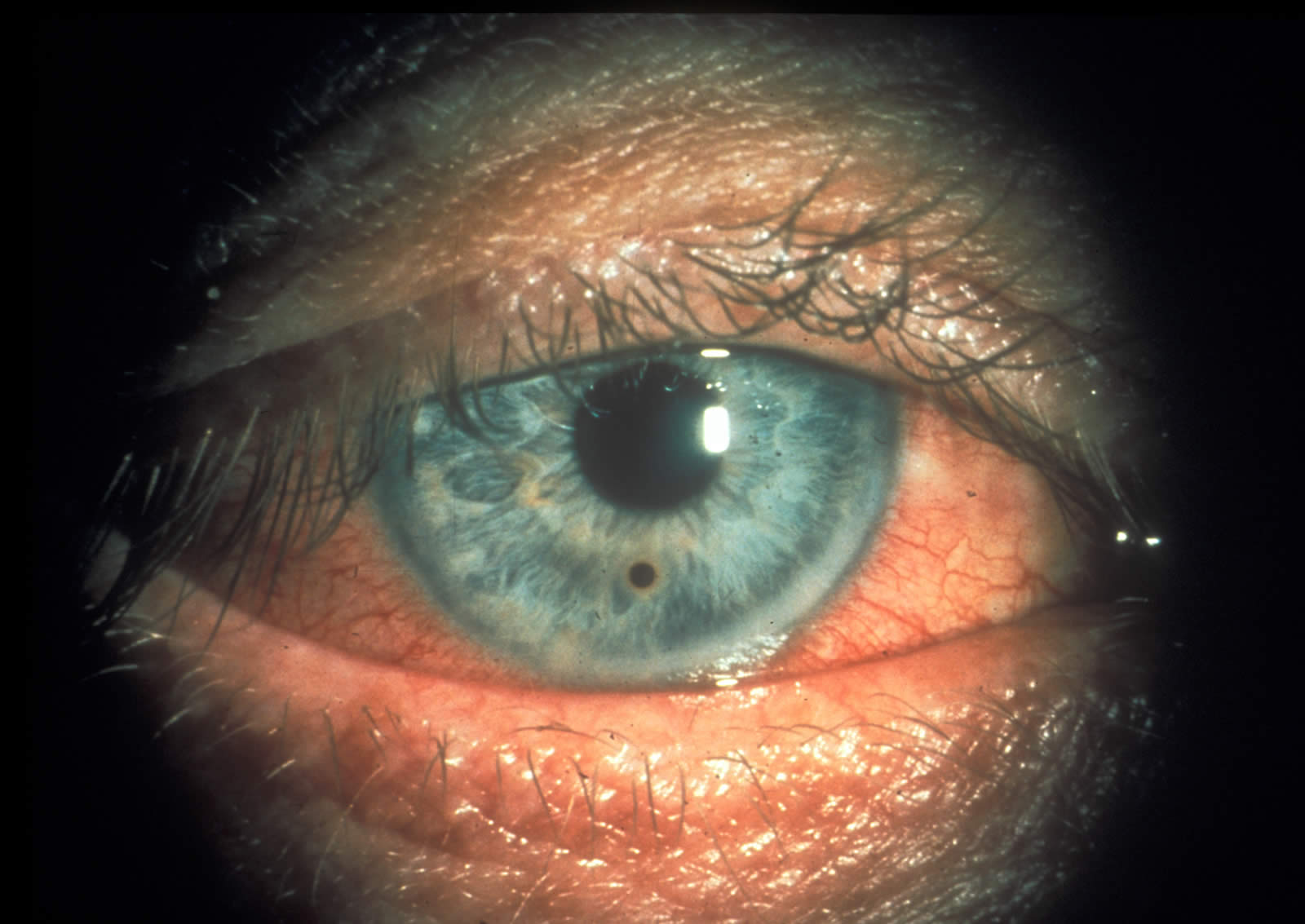
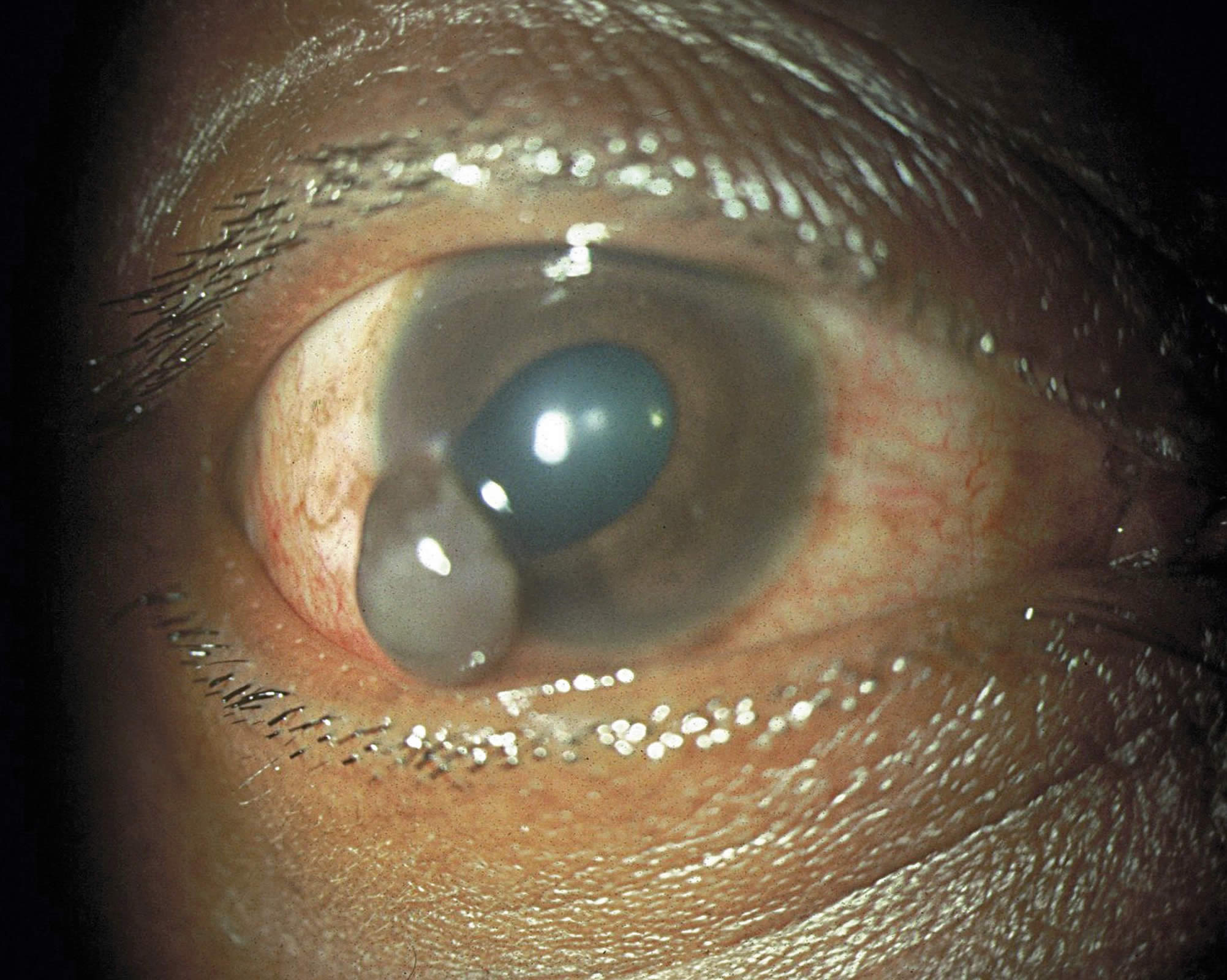
Eye injuries are common and a leading cause of preventable unilateral blindness worldwide. The causes vary, but drawing upon experience from The Gambia and Senegal, trauma is more common during the farming season and among small-scale metal workers working without eye protection. Stick injury is common in children and farmers, sometimes causing a penetrating injury that can result in the affected eye quickly becoming infected. Blunt trauma is common among children, who can be injured with a catapult or stone. The dusty environment is a common cause of corneal, conjunctival and sub-tarsal foreign bodies injuries.
Injuries are often preventable which makes education at the community level important. Village health workers and community-based volunteers (such as ‘Nyateros‘ or ‘Friends of the Eye’ in The Gambia) are important promoters of good eye health practices.
A network of community ophthalmic nurses can provide appropriate first aid and refer from village level to secondary or tertiary care. This can significantly reduce visual impairment and blindness resulting from injuries. Health facilities should be ready to deal with eye injuries by:
-
ensuring that staff know how to assess eye injuries and perform basic first aid procedures appropriate to their level of training
-
ensuring a supply of equipment, drugs and consumables required to assess and provide first aid for eye injury
-
having a plan of how to refer patients, including nearest referral facilities, and options for transporting patients in an emergency.
The chart below provides an easy reference for community level workers faced with an eye injury in their clinic or community.
First aid management of eye injuries
Cause of injury
|
Burns |
Foreign body (FB) |
Blunt injury |
Penetrating injury |
Lid laceration |
|
|---|---|---|---|---|---|
|
Variations |
Chemical, thermal or radiation |
Conjunctival, corneal or |
Blood in anterior chamber (Hyphaema) |
Corneal or scleral perforation |
Laceration of lid margin or |
|
Pain |
Severe |
Mild/moderate |
Mild/moderate |
Severe |
Moderate |
|
Vision |
Reduced |
Vision affected if central cornea involved |
Reduced |
Reduced |
Normal |
|
Torch examination |
Red eye and hazy cornea |
FB seen on conjunctiva, cornea or under lid |
Blood seen in anterior chamber. Pupil may be dilated |
Cornea hazy and pupil may be distorted with uveal prolapse. Shallow anterior chamber |
Laceration visible |
Management
|
Burns |
Foreign body (FB) |
Blunt injury |
Penetrating injury |
Lid laceration |
|---|---|---|---|---|
|
First Aid |
Remove |
Assess |
Urgent |
Refer |
|
Immediately irrigate thoroughly with clean water with special attention to particles that may be trapped under the eyelid. Apply antibiotic eye ointment and refer to eye unit immediately |
Remove with edge of clean cloth. If on cornea, gently use matchstick covered with cotton wool. Refer if embedded |
Rest; refer if hyphaema is severe or no improvement with bed rest by day three. Analgesics must not contain aspirin |
Refer immediately to an eye unit.Tetanus toxiod 0.5ml immediately |
Refer to an eye unit to ensure proper alignment of the lid margin. Tetanus toxoid 0.5ml immediately |